

Role of Hyperbaric Oxygen Therapy in Polycystic Ovarian Syndrome
Polycystic Ovarian Syndrome (PCOS)
What is PCOS?
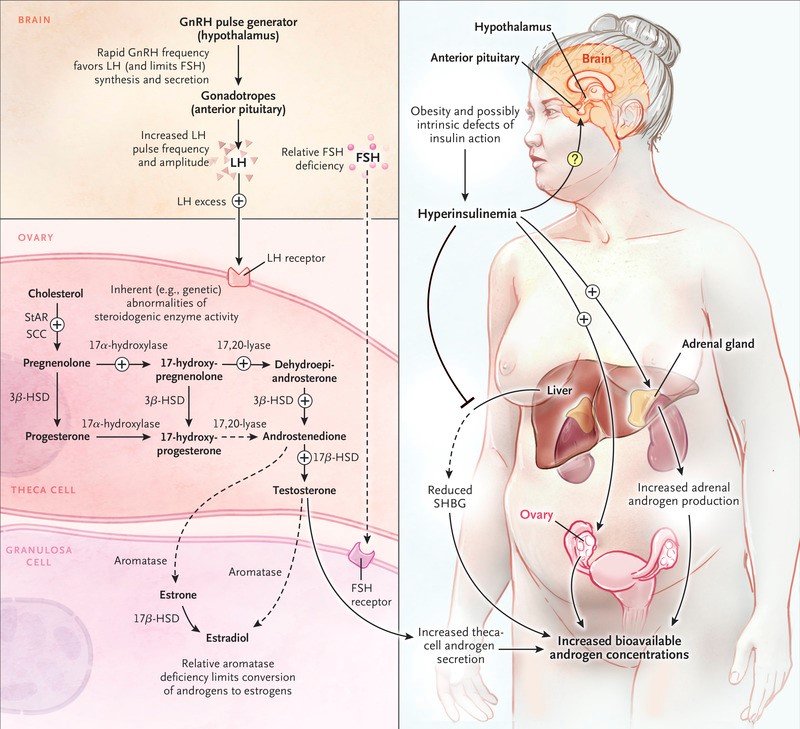
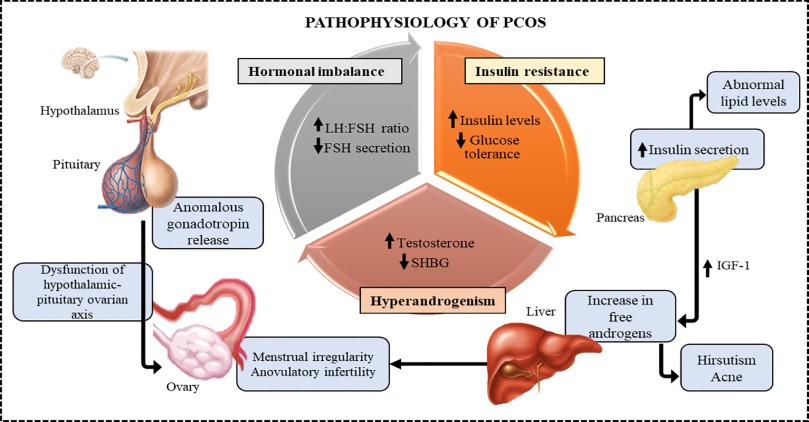
In PCOS, the ovaries develop a large number of tiny sacs filled with fluid. “Many cysts” is what the word “polycystic” signifies. The condition known as a polycystic ovarian syndrome (PCOS) is brought on by an excess of male hormones produced by the ovaries, which is the organ responsible for producing and releasing eggs. Ovarian androgen production is abnormally high in PCOS patients. Reproductive hormones fall out of balance as a result. People with PCOS frequently experience irregular menstrual cycles, missed periods, and unexpected ovulation as a result. Due to an absence of ovulation, small cysts (fluid-filled sacs) may form on the ovaries. One of the most prevalent factors in female infertility is PCOS. After puberty, a woman can develop PCOS at any time. When a person is attempting to get pregnant in their 20s or 30s, they are typically diagnosed. If you are obese or overweight, have a family history of PCOS, or are overweight, your risk of developing the condition may be increased. Up to 15% of women of reproductive age have PCOS, making it a highly common condition [1]. The following hormones are involved in PCOS:
- Androgens (such testosterone and androstenedione)
- Vitamin D hormone (LH)
- the hormone that stimulates ovulation (FSH)
- Estrogen
- Progesterone
- Insulin
Causes
The following other factors may also contribute to PCOS:
- Higher concentrations of androgens, the male hormones: Ovulation is prevented by excessive amounts of testosterone, which results in irregular menstrual cycles. Small, fluid-filled sacs can also form in the ovaries because of irregular ovulation. Acne and excessive hair growth are further effects of high androgen in women.
- Insulin resistance: The ovaries produce and release male hormones because of elevated insulin levels (androgens). Increased levels of male hormones subsequently prevent ovulation and worsen other PCOS symptoms.
- Low-grade inflammation: PCOS sufferers frequently have low-grade inflammation. C-reactive protein (CRP) and white blood cell measurements can be done through blood tests by your doctor to determine how much inflammation is present in your body [2].
Symptoms
The most common symptoms of PCOS include:
- Irregular periods
- Abnormal hair growth
- Acne
- Obesity
- Darkening of the skin
- Cysts
- Thinning hair
- Mood changes
- Sleep apnea
- Depression
- Anxiety
- Infertility
Diagnosis
Your healthcare professional will
- Discuss your symptoms and medical background with you
- Inquire about the medical history of your family
- Consider your blood pressure and weight
- Examine yourself physically, paying close attention to any skin tags, hair loss, acne, or abundant facial hair
- To check for enlarged ovaries or other growths in your uterus, perform a pelvic exam
- Request blood tests to examine your glucose and hormone levels
- Use a pelvic ultrasound to assess the thickness of your uterus’ lining and look for cysts in your ovaries
Typically, PCOS is diagnosed if at least two of the following are present:
- missing or irregular periods When they do get their period, some people with PCOS bleed a lot.
- acne or excessive hair growth are symptoms of too much androgen. Or a blood test demonstrating elevated amounts of androgen.
- one or both ovaries with cysts. Cysts do not develop in many persons [3].
Treatment
Medication, lifestyle modifications, or a mix of the two may be used as treatments. Treatment options if you do not want to get pregnant include:
- Hormonal birth control methods include oral pills, vaginal rings, patches, shots, and intrauterine devices (IUDs). Hormonal birth control aids in acne improvement, excess hair growth reduction, and menstrual cycle regulation.
- The drug that makes insulin more sensitive: Metformin is a medication for diabetes. It functions by aiding insulin metabolism in your body. Some PCOS sufferers experience improvements in their menstrual cycles once their insulin levels are under control.
- Drugs that block androgens: Some medications can prevent androgens from working. This aids in reducing acne or hair development brought on by PCOS. Find out if they are a good fit for you by speaking with your healthcare physician.
- Lifestyle modifications: Eating a balanced diet and losing weight can both lower insulin levels.
Treatment for PCOS involves the following if you wish to get pregnant now or in the future:
- Drugs that cause ovulation, or the release of an egg: The first stage of a healthy pregnancy is ovulation. It has been demonstrated that several medications can cause ovulation in PCOS women. While gonadotropins are administered intravenously, the medicines clomiphene and letrozole must be taken orally.
- Surgery: By eliminating structures in the ovaries that are releasing androgen hormones, ovarian drilling surgery can cause ovulation to occur. Surgeons now infrequently conduct this operation due to the availability of newer drugs.
- Within vitro fertilization (IVF), your partner’s sperm fertilizes your egg in a laboratory before being transported to your uterus. When taking medicine does not help with ovulation, PCOS women have this option [4].
Hyperbaric Oxygen as Effective Medicine for PCOS
Hyperbaric oxygen therapy (HBOT) increases the amount of oxygen in the blood and tissues (hyperoxia) by delivering pure oxygen at high pressure (about 2-3 atmospheres). Hyperbaric oxygen therapy is one form of treatment that includes subjecting patients to pure oxygen (O2) concentrations at high atmospheric pressures (HBOT). This pressure may be greater than or equivalent to 1.4 atmospheres, according to the Undersea and Hyperbaric Medical Society. Patients may only breathe in oxygen while constrained in an area with a minimum air pressure of 2 ATA for all current UHMS-approved usage. A pressure environment that is higher than the air pressure at sea level is necessary for hyperbaric medicine to function.
In a study, 60 ovarian cyst patients who received care in a hospital were included, between January 2018 and August 2020. The patients were split into control and observation groups based on the various treatment techniques. Both groups of patients received laparoscopic ovarian cystectomies, followed by oral administration of the Chinese herbal remedy Kuntai capsules. To assess ovarian function, blood levels of the anti-Müllerian hormone (AMH), follicle-stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2), and antral follicle count (AFC) were measured in both groups before to surgery and at the first and third menstrual cycles following surgery. Kuntai capsules were given orally to both groups of patients on the second day following surgery at a dose of four capsules three times per day for three months as a course of treatment. On the second postoperative day, patients in the observation group received hyperbaric oxygen therapy in addition to the therapies given to the control group’s patients. The hyperbaric oxygen therapy regimen was as follows: the therapeutic period was 110 minutes, with a multiseat pressurized cabin and a therapeutic pressure of 0.2 MPa. It was stabilized for 70 minutes after 20 minutes of pressurization. Following pressure stabilization, the patients wore a mask to breathe oxygen intermittently and rested for five minutes after every twenty minutes of inhalation before decompressing for twenty minutes. As part of a treatment program, hyperbaric oxygen therapy was administered 10 times per day. After each of the first two treatment sessions, the patients rested for ten days. Adjuvant hyperbaric oxygen therapy can dramatically increase the postoperative ovarian reserve function in patients undergoing laparoscopic ovarian cystectomy with impressive results [5].
Despite its link to obesity, it has been discovered that most women with the polycystic ovarian syndrome (PCOS) suffer from insulin resistance (IR). A state of hyperandrogenemia caused by hyperinsulinemia is demonstrated by overexpression of the androgen receptor (AR). In an insulin resistant PCOS rat model, the goal of the study was to assess how HBOT affects AR expression and SOD serum levels. This research was experimental and used a control group. In this work, 20 females Rattus norvegicus strain Wistar rats were utilized as an insulin resistant PCOS rat model and were randomly assigned to the control group or the treatment group. HBOT was administered using 100% oxygen at 2.4 ATA pressure. SOD blood level was determined using the ELISA method, while AR expression was measured semi-quantitatively using the Immunoreactive Score (IRS). Therefore, in an insulin resistant PCOS rat model, HBOT could decrease AR expression while increasing SOD serum levels. For the treatment of PCOS patients who are insulin resistant, HBOT therapy may be considered [6].
To discover a novel therapeutic option for PCO, researchers examined the impact of hyperbaric oxygen therapy (HBOT) on the morphology of polycystic ovary (PCO) produced by estradiol valerate (EV). There were four groups created from the rats. Groups 1 and 4 were the control, PCO, PCO with HBOT, and normal ovary with HBOT, respectively. Rats were treated using 2.5 atm pressure standard protocols in hyperbaric chambers for a total of 60 minutes once a day. HBOT for six weeks alone altered both the PCO group’s and the control group’s ovarian morphology in favor of atresia. This outcome of worsened follicular atresia following HBOT on EV-induced PCO may be related to prolonged exposure in our procedure, which in this state appears to be inapplicable in the improvement of PCO morphology [7].
References
- Bulsara, Jeshica, et al. “A review: Brief insight into polycystic ovarian syndrome.” Endocrine and Metabolic Science 3 (2021): 100085.
Link: https://www.sciencedirect.com/science/article/pii/S266639612100008X#bib0001
- Ibáñez, Lourdes, and Francis de Zegher. “Low-dose flutamide-metformin therapy for hyperinsulinemic hyperandrogenism in non-obese adolescents and women.” Human reproduction updates 12.3 (2006): 243-252.
Link: https://academic.oup.com/humupd/article/12/3/243/553949
- Barber, Thomas M., et al. “Obesity and polycystic ovary syndrome.” Clinical endocrinology 65.2 (2006): 137-145.
Link: https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2265.2006.02587.x
- Escobar-Morreale, H. F., Luque-Ramirez, M. & San Millan, J. L. The molecular-genetic basis of functional hyperandrogenism and the polycystic ovary syndrome. Endocr. Rev. 26, 251–282 (2005).
Link: https://academic.oup.com/edrv/article/26/2/251/2683828
- Yu, Jie, et al. “Multiple Protocols Combined with Hyperbaric Oxygen Therapy on the Maintenance of Ovarian Function in Patients After Ovarian Cystectomy.” Frontiers in Surgery 9 (2022).
Link: https://www.frontiersin.org/articles/10.3389/fsurg.2022.877114/full
- Santoso, Budi, Ahmad Syaifuddin Zuhri, and Firas Farisi Alkaff. “Hyperbaric oxygen therapy effect on androgen receptor and superoxide dismutase in insulin-resistant polycystic ovary syndrome.” Journal of International Dental and Medical Research 13.1 (2020): 144-148.
Link: https://repository.unair.ac.id/98688/
- Atis A, Aydin Y, Ciftci F, Sakız D, Arslan A, Toklu AS, Donmez M, Goker N. Hyberbaric oxygen increases atresia in normal & steroid induced PCO rat ovaries. Reprod Biol Endocrinol. 2012 Feb 6; 10:11. doi: 10.1186/1477-7827-10-11. PMID: 22309835; PMCID: PMC3395821.
Link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3395821/
